
ANEURISMAS SACULAR E FUSIFORME TRATADOS POR IMPLANTE DE ENDOPRÓTESE E EMBOLIZAÇÃO COM MOLAS.
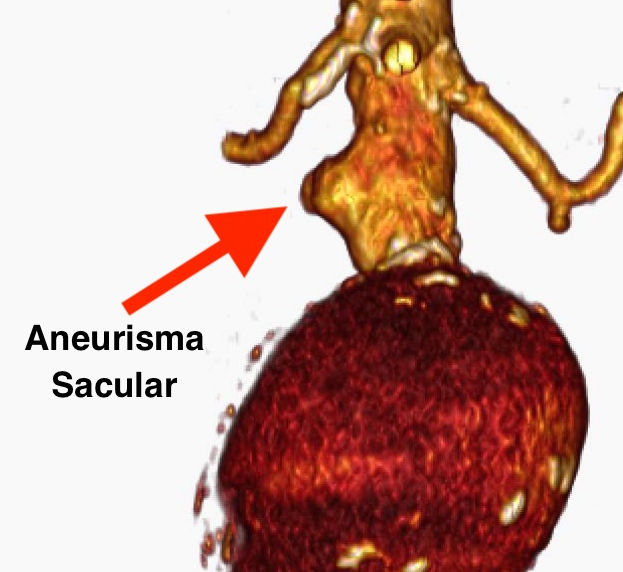
Relato um caso de um grande aneurisma fusiforme acompanhado de um aneurisma sacular restrito ao segmento do colo. O colo apresentava pequena zona de ancoragem proximal e distal ao aneurisma sacular, assim, optou-se pelo tratamento com implante de endoprótese seguido do preenchimento com molas do saco aneurismático sacular. A compactação com molas do aneurisma sacular foi escolhida pelo receio de ruptura deste, em havendo no futuro um endoleak tipo I não detectado precocemente.
Para tal, foi posicionado previamente, via braquial direita um cateter Vertebral 5F no aneurisma sacular antes da liberação da endoprótese.
Após a liberação completa da endoprótese Nano Endoluminal e suas extensões ilíacas (corpo principal – 31X14X14X170, extensão Ilíaca esquerda 16X16X130 e extensão Ilíaca direita 16x16x8), procedeu-se a compactação do aneurisma sacular utilizando-se 5 molas fibradas Concerto 20mm x 50cm Medtronic entregues via Microcateter Rebar Meditronic pela luz do cateter Vertebral 5F.
As angiografias de controle imediato e o eco-Doppler de controle 30 dias após evidenciaram a oclusão de ambos os sacos aneurismáticos.
Procedimento semelhante foi por nós realizado e publicado no Jornal Vascular Brasileiro em 2013 (J Vasc Bras. 2013 Out.-Dez.; 12(4):308-311) em 2013.
Acessível no link: https://www.scielo.br/j/jvb/a/YxkTb4x3r4hCPdGYxKrP9sL/?lang=pt
Vamos seguir acompanhando a evolução com ultrassom a cada semestre, e com angio-TC se necessário.
Aneurismas sacular e fusiforme tratados por implante de endoprótese e embolização com molas
SACULAR ANEURYSM ASSOCIATED WITH A LARGE FUSIFORM ANEURYSM TREATED BY IMPLANTATION OF A ENDOPROSTHESIS AND EMBOLIZATION WITH COILS.
I report a case of a large fusiform aneurysm accompanied by a saccular aneurysm restricted to the neck segment. The neck had a small area of anchorage proximal and distal to the saccular aneurysm, so treatment with endoprosthesis implantation was chosen followed by filling the saccular aneurysmal sac with coils. The compression of the saccular aneurysm with coils was chosen due to the fear of its rupture, in the event of a type I endoleak not detected early in the future.
For this purpose, a 5F Vertebral catheter was previously positioned via the right brachial artery in the saccular aneurysm before releasing the endoprosthesis. After complete release of the Nano Endoluminal endoprosthesis and its iliac extensions (main body – 31X14X14X170, left iliac extension 16X16X130 and right iliac extension 16x16x8), the saccular aneurysm was compacted using 5 Concerto coils 20mm x 50cm Medtronic delivered via Microcatheter Rebar Meditronic by 5F Vertebral Catheter lumen.
The immediate control angiography and the control ultrason Doppler 30 days later showed the occlusion of both aneurysmal sacs.
A similar procedure was carried out by us and published in the Jornal Vascular Brasileiro in 2013 (J Vasc Bras. 2013 Oct.-Dec.; 12(4):308-311) in 2013 and accessible in English version through this link. https://www.scielo.br/j/jvb/a/YxkTb4x3r4hCPdGYxKrP9sL/?lang=en
We will continue to monitor the evolution with ultrasound every six months, and with CT angiography if necessary.